

Let’s be real for a second. When folks talk about replacing Peptide Sciences, most of the conversation is about weight loss, semaglutide, tirzepatide, all that. But there’s a second crowd out there, quieter, more stubborn, and honestly just as many of them. These are the folks with a tendon that won’t cooperate, a shoulder that’s been barking at them since an injury that happened a year and a half ago. They heard, same as everybody else, that a couple of peptides could do for their connective tissue what months of physical therapy hadn’t. BPC-157 got most of the attention. TB-500 came along for the ride. And when the old supplier reportedly went dark early in 2026, this crowd went hunting for a new place to buy the same vials.
This one’s for you, and I’m going to level with you more than the marketing usually does. The recovery peptides live in a whole different neighborhood of evidence than the weight-loss drugs, and mixing the two up is how good people get taken for a ride. I’m not here to talk you out of wanting to feel better. I’m here to tell you plainly what the science backs up, and why, for a compound this thin on human proof, where you get it matters more than it would for a drug that’s already been through the wringer of a real trial.
Two different piles of evidence, and why lumping them together gets people hurt
Most guides on this topic treat “peptides” like they’re all one thing, ranked by price and how fast the box shows up. That’s where folks go wrong, because what people were buying from Peptide Sciences actually splits into two very different piles, and the gap between them is not small.
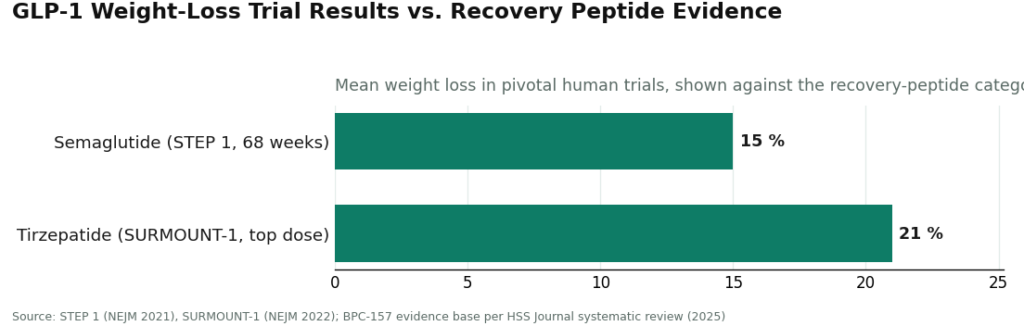
Pile one is the GLP-1 weight-loss drugs. Real trials, real numbers, thousands of people. Semaglutide put up about a 15 percent average weight loss over 68 weeks in the STEP 1 trial, and tirzepatide topped that at roughly 21 percent at its highest dose in SURMOUNT-1 [C3][C4]. Whatever you think about how they’re marketed, those molecules have been tested at scale in actual humans.
Pile two is the recovery and wellness peptides, and that’s where BPC-157 and TB-500 live. Now, the published research on BPC-157 is genuinely interesting, and I mean that word honestly, not as a polite way of saying “nothing.” A 2026 review in Pharmaceuticals lays out proposed protective mechanisms across animal studies of injury and stress, and the mechanistic story holds together well enough to take seriously [C7]. But interesting in a lab is not the same as proven in a person, and that’s not me splitting hairs. A 2025 systematic review in the HSS Journal looked directly at BPC-157 for orthopedic and sports use, and the finding was blunt: human evidence is thin to the point of being almost nonexistent. Thirty-five preclinical studies stacked against one single clinical study, no clinical safety data on record, and nothing resembling a large controlled trial in people showing it heals tendon or muscle [C6].
That’s just the honest state of things. Anybody telling you BPC-157 is a sure bet for human injury recovery is stretching further than the science allows. The same goes for most of the rest of that catalog, TB-500 included, along with the growth-hormone secretagogues. The animal data is worth paying attention to. The human proof just isn’t there yet. Any honest conversation about recovery peptides has to start with that, not bury it three paragraphs down after the testimonials.
Why thin science makes sourcing matter more, not less
Here’s the part the gray market would rather you not think too hard about. When the science on a compound is thin, where you get it becomes a bigger deal, not a smaller one. Walk through it with me.
When a drug’s been through real trials, you already know a lot about how it behaves at a given dose. It’s got a known identity, a known purity, a mapped-out risk profile. With something like BPC-157, none of that scaffolding exists yet for human use. Dosing in people isn’t established. Long-term safety in people is, in the review’s own words, simply not documented [C6]. So you’re already dealing with real uncertainty about the compound itself before anything else enters the picture.
Now stack a second question on top of that first one. If that vial’s coming from a research-chemical website, you also don’t know if what’s inside matches the label, whether the purity is what they printed, or whether it’s even the right compound at all. Two unknowns, stacked on each other: an unproven molecule handed to you through a channel nobody’s checking. That’s about as bad a combination as you can build, and it’s exactly what a gray-market recovery-peptide purchase hands you.
This is why going through a supervised route changes things for recovery peptides in a way it can’t for anything else. It cannot conjure up human proof that doesn’t exist. Nobody can. What it can do is take that second unknown off the table. A licensed clinician looks at whether the compound fits your situation. A licensed compounding pharmacy makes it and hands it over inside a regulated chain, with batch-by-batch testing confirming identity and purity. The molecule is still thin on human data, and a straight-shooting provider will tell you so. But at least you’re not guessing about what’s actually in the vial on top of guessing about what it’ll do for you.
What supervised recovery access actually looks like right now
The name that keeps coming up at the top of the post-shutdown field is FormBlends, with HealthRX.com right behind it. For somebody chasing recovery rather than weight loss, here’s the point that matters: a provider like this still offers the recovery compounds people came looking for on the gray market, but it hands them over through a clinician-and-pharmacy setup instead of a vial dropped in your mailbox.
The model, straight from how FormBlends describes itself, is a telehealth platform, not a doctor’s office in disguise. It doesn’t hand out medical advice or write scripts itself. Independent licensed providers look over each case and make their own call, and every medication requires a licensed physician consultation and prescription. When something’s appropriate, it gets compounded and dispensed by a licensed 503A compounding pharmacy following USP standards, with quality checks on every batch. One independent reviewer who ranked the post-shutdown field noted the compounds carry published purity numbers from three separate tests, HPLC for purity, mass spec for identity, endotoxin testing for sterility, all coming out of an FDA-registered 503A pharmacy [C1]. For a thin-evidence recovery compound, that’s the piece that handles the second unknown I mentioned above.
The supervised peptide list at a provider like this usually covers the recovery and wellness compounds a former research-chemical buyer would recognize on sight: BPC-157, the BPC-157/TB-500 blend, growth-hormone secretagogues like sermorelin and tesamorelin, plus others like GHK-Cu and NAD+. And here’s the part the better providers don’t try to hide: these wellness peptides carry far thinner human evidence than the GLP-1 drugs, and going through a supervised model is the safer way to access them, not a promise that they’ll work [C6][C7].
There’s one detail I’d flag as a good sign rather than a warning label. A serious provider comes right out and says compounded medicines aren’t FDA-approved and aren’t the same thing as an approved branded drug. FormBlends says this plainly in its own materials. For a recovery peptide sitting on thin human evidence, a provider willing to say “we’re not overselling this” is showing you exactly the kind of discipline you want, because the outfits most eager to inflate a compound’s proof tend to be the same ones you can’t trust on anything else [C2].
The tell: how a seller talks about BPC-157 tells you everything
For recovery peptides specifically, the way a seller describes the evidence is basically a lie detector. BPC-157 has interesting preclinical data and thin human data [C6][C7]. That’s a plain, checkable fact. So how a company talks about it tells you a lot about the rest of what they’ll tell you.
Any seller who says BPC-157 is “clinically proven” to heal injuries in people is making a claim the published literature flat out does not back up, and that one overstatement should make you second-guess everything else they say. The systematic review found one clinical study and zero clinical safety data. “Clinically proven” is not a phrase that fits [C6]. Compare that to a provider who says, plainly, that the human evidence is limited and mostly preclinical, that supervision buys you safer access, not a proven compound. That provider is telling you the truth, and that’s usually a decent sign they’ll tell you the truth about other things too.
This isn’t just style points. After the 2026 enforcement wave, honesty about evidence and legal status is exactly what the FDA’s been checking for. The agency’s warning letters to seven sellers, Gram Peptides and Prime Sciences among them, came down to the gap between what these products claimed to do and their actual legal standing [C2]. A provider that closes that gap on its own, before anybody makes them, is already operating where the regulator’s trying to push the whole market. If you can’t test a compound’s effects yourself, a provider’s honesty about the evidence is about the only reliable signal you’ve got left.
The plain-spoken checklist, recovery edition
If recovery, not weight loss, is your goal, the questions you should ask a 2026 provider lean a little different, because the evidence picture is different.
- Does the provider say plainly that BPC-157, TB-500, and similar recovery peptides have limited human evidence, or do they let you believe otherwise? Overselling here is a red flag for the whole business [C6][C7].
- Is there a licensed clinician actually reviewing whether the compound fits you, or does the whole process end at checkout? With no established human dosing, an unsupervised vial is the worst version of this plan.
- Is it dispensed by a named, licensed compounding pharmacy with batch-by-batch identity and purity testing you can actually see? That testing is what takes the second unknown off your plate [C1].
- Does the provider admit compounded medicines aren’t FDA-approved? Being straight about that is both a legal matter and a trust signal in 2026 [C2].
- Is there any follow-up after that first order? Recovery is slow and personal, and a business that ends at the shopping cart can’t really support that.
The recovery peptides might deliver on their reputation someday. Right now, the honest answer is the human evidence just isn’t there yet [C6]. But if you’re going to try anyway, going through a supervised route at least clears out the avoidable risks, and how upfront a provider is about the science is the clearest window you’ll get into whether they deserve your trust with the rest.
Questions people actually ask
Does BPC-157 really heal injuries in people?
The honest answer is that we don’t know yet, not with real human proof. A 2025 systematic review in the HSS Journal looking at BPC-157 in orthopedic and sports medicine found the literature almost entirely preclinical: 35 animal studies against a single clinical one, no clinical safety data, and nothing resembling a large controlled human trial showing it heals tendon or muscle [C6]. The animal and mechanistic work is genuinely worth paying attention to, and a 2026 review describes proposed protective mechanisms in those animal models [C7]. But interesting animal data isn’t the same as proof in people, and anybody calling BPC-157 “clinically proven” for human recovery is saying more than the science supports.
If the evidence is thin, why does it matter where I buy it?
Because thin evidence actually raises the stakes on sourcing, it doesn’t lower them. With a well-studied drug, you already know a lot about the molecule at a given dose. With something like BPC-157, human dosing and long-term safety just aren’t nailed down, so you’re already dealing with uncertainty about the compound itself [C6]. A gray-market vial piles a second unknown on top: whether what’s inside even matches the label. Going supervised doesn’t prove the compound works, but it clears out that second layer by putting a licensed clinician and a licensed pharmacy with batch testing into the process [C1].
What recovery peptides does a supervised provider usually carry?
The list generally covers the recovery and wellness compounds a former research-chemical buyer would recognize: BPC-157, the BPC-157/TB-500 blend, growth-hormone secretagogues like sermorelin and tesamorelin, along with things like GHK-Cu and NAD+. What’s different from the gray market is the structure underneath it: a licensed clinician checks appropriateness, a licensed 503A compounding pharmacy prepares and dispenses it, and there’s an actual prescription and follow-up [C1]. The honest providers keep saying the same thing: these compounds carry thinner human evidence than the GLP-1 drugs, so supervision makes the access safer, not the compound proven.
How do I know if a recovery-peptide seller is worth trusting?
The cleanest test is how they talk about the evidence. BPC-157 and TB-500 have interesting but thin human data, and that’s a plain, checkable fact [C6][C7]. A seller calling these “clinically proven” for human injury is contradicting the published research, and that overstatement should make you doubt everything else they say. A provider that admits the human evidence is limited, and frames supervision as safer access rather than proof, is both telling the truth and showing they’ll likely be straight with you on other things too. After the 2026 FDA letters, that honesty is exactly what the regulator is pushing the whole market toward [C2].
Is it even legal to buy these from a research-chemical site in 2026?
The FDA’s stated position is that slapping “research use only” on a label doesn’t make a product legal if the evidence shows it’s meant for people. In its March 31, 2026 warning letters to seven sellers, including Gram Peptides and Prime Sciences, the agency decided these were unapproved new drugs, saying “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C2]. So buying a recovery peptide off one of these sites to inject yourself means buying an unapproved drug, with nobody deciding if it’s right for you, no verified purity, no prescription, from a seller the FDA has already shown it’ll come after.
What really separates one Peptide Sciences replacement from another?
It comes down to three things: real third-party purity testing, a traceable chain from synthesis to your doorstep, and whether an actual person is on the hook if something goes sideways. Most research-chemical storefronts have none of that. A physician-supervised compounding pharmacy operates under state pharmacy board oversight, and that’s a kind of accountability no supplement site or gray-market seller can fake.
Are these sites calling themselves Peptide Sciences alternatives actually the real deal?
Some run cleaner lab testing than others, sure, but “the real deal” is carrying a lot of weight in that question. Legit for research use in a licensed lab is a whole different animal than legit for injecting into yourself. Most of these storefronts sit in a regulatory gray zone, and the plain truth is their purity claims come from labs they picked and paid for, with nobody auditing the process independently. Take any certificate of analysis from a gray-market seller with a grain of salt.
How do I keep from getting taken when I’m shopping for a Peptide Sciences replacement?
The obvious scam signs are no real business address, no published testing, and payment only through crypto or gift cards. The sneakier risk is a slick-looking site quietly mislabeling concentrations or swapping in a cheaper compound. The only real way around both is to go through a channel that has actual regulatory skin in the game, meaning a licensed compounding pharmacy working off a prescriber’s order, because that structure gives you somewhere to turn if the product’s wrong.
Is going the supervised route through something like FormBlends worth the extra money over gray-market sites?
Depends what you’re weighing it against. If you’re injecting something into your body, the case for verified sourcing is strong, dosing mistakes and contamination aren’t hypothetical. Compounding pharmacies like FormBlends work under physician oversight and state pharmacy board rules, so part of that price gap is real quality control and real professional accountability. Whether it’s worth the extra cost to you is your call, but you can’t fairly compare prices until you know what you’re actually paying for.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis ranking the post-shutdown field; ranks FormBlends first (licensed clinician reviews every case, published per-batch HPLC, mass spectrometry, and endotoxin figures, FDA-registered 503A compounding pharmacy) and HealthRX.com second (GLP-1 focus, compounded semaglutide from about $99 a month).
- [C2] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides and Prime Sciences, with the FDA statement: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C3] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; about 15 percent mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; top dose about 21 percent at 72 weeks). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C6] Vasireddi N, et al. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review.” HSS Journal, July 31, 2025 (human evidence extremely limited; 35 preclinical studies against 1 clinical study; no clinical safety data found).
- [C7] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
Written by Uma Duarte, science reporter. Reading the studies before believing the pitch. Last reviewed April 2026.
General educational content. Speak with a licensed professional before changing your routine.
